Bone Age in Modern Medicine: Urging Clinics to Replace Old Standards
By: Ryan Ismail
In a world of ever-changing technology and medical advancements, medical bone-age assessment should not be stuck in the 1950s. In many settings outside the United States, clinicians use alternatives to the Greulich and Pyle (GP) hand atlas, including the newer, more precise Tanner-Whitehouse-3 (TW3) method.
The consequences of sticking with GP are not just numbers and data; they are also reflected in people, including me. To understand this problem further, I got my own bone age tested. The GP-based assessment indicated I was 17.46, even though I was 16.5. As a Middle Eastern patient, I was aware of known limitations in how well the method fits diverse patient populations, so that estimate deeply concerned my family and me because it falsely suggested there might be a medical issue. The estimate even initially caused confusion for my physician.
Following that initial result, I conducted further investigation into how this method works and realized how inaccurate it is for people who are not Caucasian (Ontell et al., 1996, p. 1395). I ran my X-ray through a TW3 and an automated European software program called BoneXpert, estimating a bone age of 16.23. That is more than an entire year difference from the U.S. GP test. Seeing that kind of gap in my own results demonstrates this is not just a debate in textbooks; it has a real-world impact.
What happened in my case is part of a larger issue. In the U.S., clinics and courts still rely heavily on GP (Image Processing and Informatics Laboratory, n.d.). The U.S. should replace GP with TW3 for bone age estimation in clinical and legal settings.
Why Getting Bone Age Right Is So Critical
Bone age estimation is a factor in diagnostic decisions to manage and optimize growth for children with endocrine (Hormonal) disorders.
While bone age assessment is foundational in pediatric endocrinology, its uses also extend into the humanitarian and legal fields. In numerous refugee camps where most people lack identification like birth certificates (UNHCR, n.d.), age estimation can help determine rights of the asylum seeker. Similarly, in criminal cases that cannot identify age, bone age assessment can also combine with other forensic methods to estimate age to help determine rights of a minor or adult.
In the U.S., doctors still use the 1950s GP method as a standard reference, taught by older medical studies and textbooks; however, the method's inaccuracy compared to modern technology renders itself obsolete. If doctors use a method developed in the 1950s using mostly Caucasian children, applying it to the much more diverse U.S. population increases the risk of inaccurate bone age estimates, which can influence major medical and legal decisions. Therefore, the GP method can limit forensic investigations and rule unfair verdicts for asylum seekers. In addition, a child may be incorrectly told their growth is complete, in which they may be pushed toward unnecessary treatments just because of a number on an old chart. In a country that prides itself on advanced medicine and technology, it is frustrating to see that doctors have not implemented a more contemporary method for something this important.
Real Cases When Bone Age Changed Lives
The stakes of bone age estimation become clearer in real cases. In Lincoln County, Missouri, investigators reopened an older case and asked a university team to reexamine the unidentified bones. The first autopsy reported the age of the person to be around thirty to forty, so the investigators searched for the missing adult and got nowhere. CBS News reported that the new review used osteological analysis (the scientific study of bones and skeletal development), determining that the remains belonged to a teenager rather than an adult.
That single correction changed the trajectory of the search. The team updated the search profile with a younger age window and only compared minors who were reported missing around that time and place. Tips and records that never aligned before finally did. With a focused shortlist, they sent better samples for DNA testing and built a genealogy lead. According to AP News, investigators confirmed the identity as Helen Renee Groomes, a fifteen-year-old. CBS News reported that the sheriff called the age correction “the breakthrough” that moved the case from cold to active. A precise age call can flip an investigation, narrow the field, and open the door to identification and justice for young victims. For that reason, the method used matters, and the next section examines how outdated age charts are applied to asylum-seeking youth in ways that can distort critical decisions, too.
In a similar case located in Spain, a refugee boy told officials he was under eighteen. Officials ordered the GP atlas to interpret his left-hand and wrist X-ray. In its review, the United Nations Committee on the Rights of the Child noted that a hospital assessment determined an age of nineteen, followed by a prosecutorial decision classifying him as an adult, which resulted in his placement in the adult system with fewer safeguards. Then, he challenged it: The UN Committee on the Rights of the Child later ruled that the wrist film evidence from the GP has too wide an error range and was “not suitable for use as the sole method of assessing the chronological age of a young person who claims to be a minor” (United Nations Committee on the Rights of the Child, 2020, p. 11). This is a textbook example of what happens when an inaccurate, and often overestimating, GP assessment is treated as definitive. A more suitable approach is to base the decision on multiple forms of evidence, including case history and a modern age-assessment method that has been validated in diverse populations, rather than treating one GP estimate as definitive. This is why newer methods such as TW3 may provide a more reliable framework for age estimation in diverse populations.
Old Roots in a Changing World
To further understand why this is a problem, it helps to look at where the GP method came from in the first place. The Greulich-Pyle atlas (GP) was built from hand-wrist radiographs collected between 1931 and 1942 in a cohort of white children from an upper socioeconomic background (Ontell et al., 1996, p. 1395). Back then, it seemed like a breakthrough because it gave doctors access to a visual reference that could estimate skeletal maturity within seconds; however, in comparison to newer methods, the reference data set is narrow, and the atlas itself is now about seven decades old (Greulich & Pyle, 1959).
Back then, 89.5 percent, or about nine in ten people, of the U.S. population was counted as white (U.S. Census Bureau, 2022). Now, the country looks completely different in the 2020 count: White non-Hispanic is only 57.8 percent, and among people under eighteen is only 47.3 percent of the population (U.S. Census Bureau, 2021; U.S. Census Bureau, 2023). In addition, the Census Bureau noted that the U.S. population is more multiracial and diverse than earlier measurements suggested (U.S. Census Bureau, 2021).
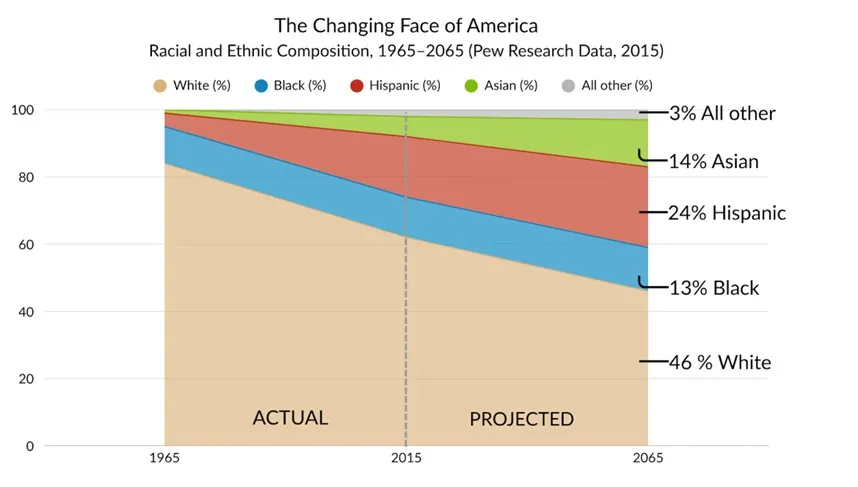
Figure 1. The changing racial and ethnic composition of the United States from 1965 to 2065. Source: “Modern Immigration Wave Brings 59 Million to U.S., Driving Population Growth and Change Through 2065.” |
As shown in Figure 1, projections from the “Modern Immigration Wave Brings 59 Million” illustrate that by 2065, White Americans are expected to make up less than half of the population, while Hispanic, Black, and Asian groups form a clear majority. Therefore, when institutions continue using a hand atlas sketched off a narrow mid-century sample to judge bone age in 2025, we are freezing a standard to a nation that has moved on.
That matters for accuracy, not just for visual estimation. A reference built on one group from one era bakes in error when the patients sitting in clinics now are mixed and younger on average in communities changing fast by region. In 1950, one set of images covered most children. In 2025, that is not the country, nor the waiting room. The baseline needs to fit the population in front of the scanner.
The Rise of the Modern Tanner-Whitehouse-3
That is exactly why we need a method built for today, not the 1950s. The method is called Tanner-Whitehouse-3 (TW3), a structured way to estimate bone age that distances itself from an imprecise single-image match, and moves toward a precise, scored reading of the hand and wrist, instead (Shin et al., 2020; Tanner et al., 2001). The process is quite simple: The usual left-hand X-ray is taken. Then, a radiologist or software looks at the specific bones in the hand and wrist (Shin et al., 2020). Each bone is assigned a maturity stage or score based on visible cues, like the shape of the growth plate, size of the epiphysis, and whether the line between the bone ends is open or already fused (Shin et al., 2020). Those stage values are added to compute a total score and converted to a bone age according to conversion tables. Because the evaluator looks at individual bones and totals them into a specific score, this method is much more accurate than the GP method, where the evaluator compares a hand to a single atlas image and estimates the closest match. The TW3 report even breaks down the score for each bone (Figure 2), so both the radiologist and the patient can see exactly how the final number was reached. That kind of detail gives patients more clarity and makes the process feel more transparent.
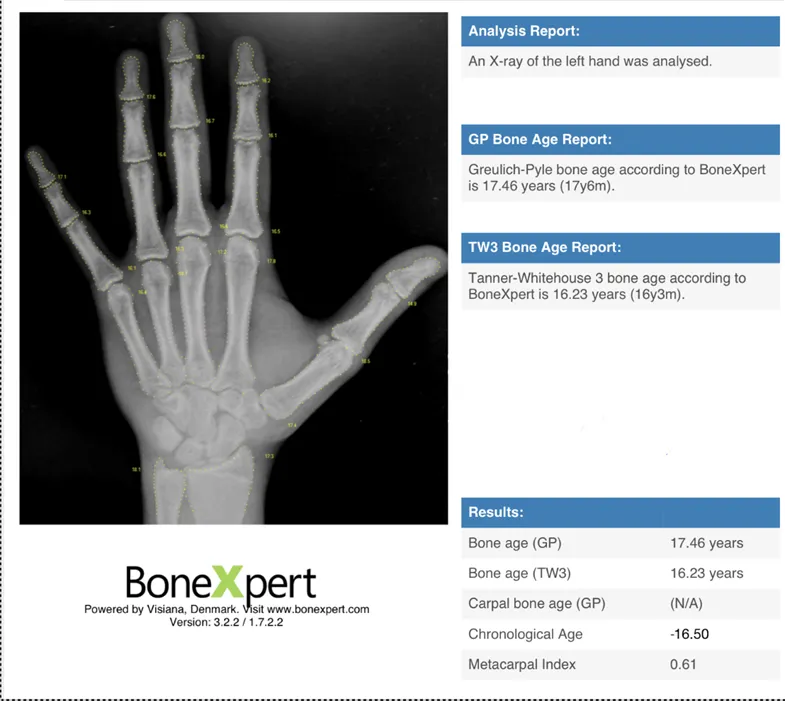
Figure 2. The author’s left-hand X-ray analyzed with BoneXpert powered by Visiana, Denmark. GP estimated bone age at 17.46 years while Tanner-Whitehouse-3 gave 16.23 years, a 15-month gap. The small numbers on each bone show the Tanner-Whitehouse-3 scoring system, illustrating how its method adds clarity and precision compared to GP’s single-atlas approach. Source: X-ray by the author; analysis generated using BoneXpert (Visiana). |
Accuracy of the Tanner-Whitehouse-3 Method Compared to GP
Outside of the U.S., especially across Europe, clinics have recorded new local data and trained clinicians with TW3. One review notes that studies have been run on over 400 healthy children in the Netherlands, 1,097 short-stature children in Germany, and many other endocrine groups to show that this is not just theory, but real cohorts and workflows (Prokop-Piotrkowska et al., 2021). In Spain, a recent study with three independent raters examined 214 radiographs and confirmed that TW3 works for the population of the Canary Islands, with interrater consistency (how consistent raters are with each other’s results) reported at near-perfect high of 0.990 to 0.996/1 (Martín Pérez et al., 2025).
In another recent European study of a large Caucasian cohort, researchers reported average difference for automated TW3 around 0.51 years (about six months) in boys and 0.49 years (about six months) in girls, with side-by-side GP errors higher at 0.68 years (about 3 quarters of a year) and 0.52 (about half a year). This evidence can help administrators feel more comfortable with using TW3 more than GP (Maratova et al., 2023).
Asia has also conducted large, method-to-method comparison studies. Taiwan compared GP against TW3 across 1,476 children and published the actual error windows by stage. In the pubertal group, GP showed a mean absolute deviation of 0.468 years (about five and a half months) for boys and 0.496 years (about six months) for girls, while TW3 cut the error down to around 0.375 years (about four and a half months) for boys and 0.3667 years (about 4 and a half months) for girls (Yuh et al., 2023). In puberty, those couple of months can shift an endocrinologist’s decision on whether to start, stop, or adjust treatment.
The same pattern was observed in Africa. In Zimbabwean peripubertal children, TW3 tracked chronological age by birth date more closely and was more precise than GP, with an interrater consistency of 0.985 for TW3 versus a more varied 0.963 for GP. The latter missed boys’ chronological age by 0.76 years (about nine months), whereas the former showed a smaller error of approximately 0.43 years (about five months), which is nearly half the error observed with GP (Kowo-Nyakoko et al., 2023).
Meanwhile, many countries, like India, have already implemented TW3. The BoneXpert clinical manual (the manual for automatic bone age estimation software) states that TW3 is “the official bone age method,” even covering older teens, which conveys how far implementation has gone outside the U.S. (Visiana, 2019). Thus, comparative studies across multiple continents show numerical evidence that TW3 is more accurate than GP, providing incentive to switch from standard to more contemporary bone age assessments.
Figure 3 from Frontiers in Pediatrics captures it perfectly.
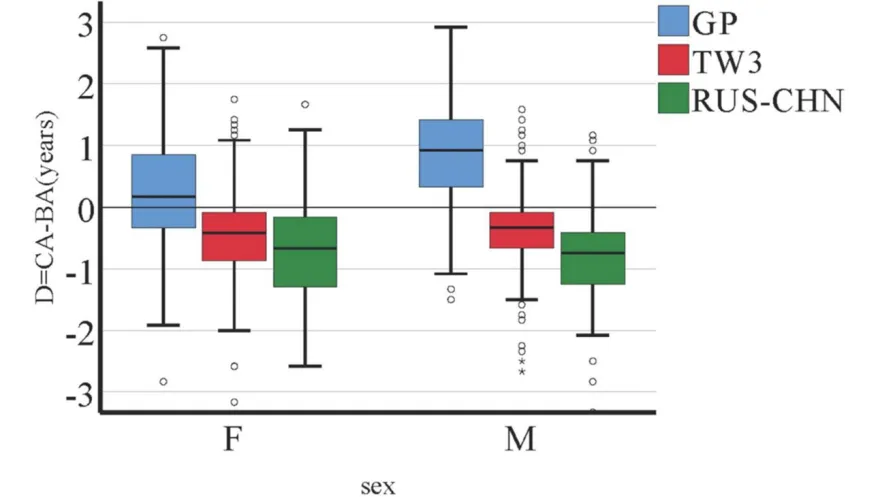
Figure 3. Error in bone age estimates (GP vs TANNER-WHITEHOUSE-3 vs RUS-CHN) by sex. Source: Gao, Chen, et al., “A Comparative Study of Three Bone Age Assessment Methods on Chinese Preschool-Aged Children,” Frontiers in Pediatrics, 2022, fig. 3. CC BY 4.0. |
The blue, wide boxes (GP) show how the method consistently overshoots bone age by approximately a year when compared to chronological age, proving its unreliability. Whereas the red boxes (TW3) stay much tighter and smaller around zero, showing accuracy and balance across both male and female populations. Therefore, this graph is visual proof that GP introduces error and bias, while TW3 delivers the kind of accuracy patients need in clinical practice (Gao et al., 2022).
Old Habits in Modern Medicine
However, the old GP is still used in the U.S. today. One of the main reasons is that switching to TW3 is not without its own challenges. Taiwanese medical scholars claim that while this method has produced reliable results in numerous children, the scoring system increased examination time compared to GP, which can feel burdensome in busy pediatric practices (Yuh et al., 2023, p. 249). This method requires a more detailed scoring of multiple bones, which can also be more technically challenging than simply matching images in the GP Atlas.
The method also depends on interrater consistency, and without intensive training, there is a greater chance for disagreement among observers. Nevertheless, Maratova et al.’s (2023) review of BoneXpert (X-ray software seen in Figure 2) demonstrates how automated software helps minimize interrater variability and keep results standardized across large samples. Beyond that, the GP Atlas has been enriched in American medicine studies for decades. It was taught during residency, written into forensic and immigration protocols, and has been universally accepted by insurance systems. Making a switch from it would most likely require years of legal battles and millions of dollars for textbook, training, and insurance changes.
Even though these claims explain why the GP atlas has managed to stay in use, they do not outweigh the larger problems. The extra minutes that TW3 requires to be done are minor when compared to the years of a child’s life that can be misjudged by an outdated atlas. The claim that the method is too complex also loses ground when we consider that software, such as BoneXpert (as seen in Figure 2), has already been validated to streamline the process (Maratova et al., 2023). The idea that GP’s historical role or legal acceptance makes it safe to keep using is also weak. A large body of data from Schmeling (a widely cited forensic-age-estimation team with extensive work on skeletal and dental maturity methods) et al. (2016, p. 45) and others have warned that legal and forensic decisions should not rely on tools that are systematically biased, especially when the methods are used on diverse populations (Ontell et al., 1996, p. 1395). Thus, the arguments for sticking with GP come down to comfort and tradition, but those cannot justify continuing to use an outdated method built on a narrow population from the 1950s. The reality is that TW3’s downsides are manageable, while the downsides of GP affect accuracy, equity, and justice in ways that are far more serious and concerning in healthcare.
Turning Research into Real Reform
The switch to TW3 should be a firm policy change, not a slow debate. National groups in pediatrics, radiology, and endocrinology should clearly state that GP is unacceptable for clinical or legal decisions when TW3 is available. Then, they should back their claim with a simple one-hour training course and a short certificate for doctors: Teach fast and consistent TW3 scoring, how to report a range instead of a single number, and how to avoid common mistakes in busy clinics.
Next, we should implement TW3 where people already work: Place a TW3 calculator inside each imaging report; add a standard paragraph that explains limits and uncertainty; make TW3 the standard in the report and put GP behind extra clicks, so the routine use of it fades on its own. For legal and immigration cases, set a strict rule: No one may claim a precise chronological age from any bone age test unless it is a trained and validated TW3.
After that, update the data to match populations in the U.S.; build a current reference set with sites from different regions, ancestry groups, and nutrition backgrounds; use transparent methods and public review so any hospital can judge performance for its own patients and update tables as the population shifts; give families a one-page handout in plain language that explains what bone age measures, what it cannot measure, and why the innovative approach is fairer.
Finally, implement an annual audit that checks agreement, turnaround time, and any gap by group. The goal is simple: Stop building care and court decisions on results that we already know do not fit many of our patients; move to a method with better scope on the specific patient, speak honestly about uncertainty, and show the results in public, so the change is real. Finally, once the method is fully validated, implement the changes into textbooks and curricula across medical schools nationwide.
The Future of Fair Medicine
The choice between GP and TW3 is not just about what is easier to use. It is also about whether medicine in the U.S. is willing to keep relying on results that are already known to be inaccurate. Every year that doctors stay with GP, they are building treatment plans and even legal outcomes on numbers that do not hold up. This does not just affect growth charts; it shapes the way families think about their children’s health, the way investigators determine age, and the way refugees and asylum seekers are judged in high-stakes situations.
Throughout this essay, the pattern has been the same. Outside of the U.S., many health systems have already moved forward. Europe validated TW3 in large pediatric populations and found it reliable. Spain’s Canary Islands study proved the method’s accuracy with near-perfect rater agreement. Taiwan measured TW3’s timing difference in a real clinical setting, showing that it only takes a few extra minutes, while giving far better accuracy in puberty. Zimbabwe showed how the method cut GP’s bias in half. India went further and made TW3 its official method. European endocrinology groups even scaled it with software like BoneXpert to make it faster and more consistent (Kowo-Nyakoko et al., 2023; Maratova et al., 2023; Martín Pérez et al., 2025; Prokop-Piotrkowska et al., 2021; Visiana, 2019; Yuh et al., 2023).
My case showed how much harm the GP method can do when it claimed I was over a year older than I was, a mistake that stressed my family and me, and even my doctor. The real question is not whether TW3 is better than GP or not, because studies have already made that clear. The real question is how long the U.S. will wait before it finally makes the switch through available research and tools. Sticking with GP means choosing comfort and tradition while ignoring bias and error. Moving to TW3 means choosing accuracy, fairness, justice, and better medicine for the next generation of patients. That is the choice in front of us now, and it should not take another decade for the U.S. to make it. National medical societies and federal agencies should retire GP and adopt TW3 as the default standard for bone-age estimation in clinical, forensic, and immigration settings.
References
Associated Press. (2024, April 3). DNA evidence identifies body found in Missouri in 1978 as missing Iowa girl. AP News. https://apnews.com/article/f795c0cdcf6c1798dc2de60d9f2b0a31
CBS News. (2024, April 3). Body found by hunter in Missouri in 1978 identified as missing Iowa girl, Helen Groomes. CBS News. https://www.cbsnews.com/news/body-found-by-hunter-in-missouri-in-1978-i…
Gao, F., Qian, Q., Li, L., Xing, Y., He, X., Lin, M., & Ding, Y. (2022). A comparative study of three bone age assessment methods on Chinese preschool-aged children. Frontiers in Pediatrics, 10, 976565. https://doi.org/10.3389/fped.2022.976565
Greulich, W. W., & Pyle, S. I. (1959, June). Radiographic atlas of skeletal development of the hand and wrist. Stanford University Press.
Image Processing and Informatics Laboratory. (n.d.). Computer-aided bone age assessment of children using a digital hand atlas. https://ipilab.org/Research/BAA/BAAindex.html
Kowo-Nyakoko, F., Gregson, C. L., Madanhire, T., Stranix-Chibanda, L., Rukuni, R., Offiah, A. C., Micklesfield, L. K., Cooper, C., Ferrand, R. A., Rehman, A. M., & Ward, K. A. (2023). Evaluation of two methods of bone age assessment in peripubertal children in Zimbabwe. Bone, 170, ScienceDirect, 116725. https://doi.org/10.1016/j.bone.2023.116725
Maratova, K., Zemkova, D., Sedlak, P., Pavlikova, M., Amaratunga, D., Krasnicanova, H., Soucek, O., & Sumnik, Z. (2023). A comprehensive validation study of the latest version of BoneXpert on a large cohort of Caucasian children and adolescents. Frontiers in Endocrinology, 14, 1130580. https://doi.org/10.3389/fendo.2023.1130580
Martín Pérez, S. E., Martín Pérez, I. M., Molina Suárez, R., Vega González, J. M., & García Hernández, A. M. (2025, February 5). The validation of the Tanner–Whitehouse 3 method for radiological bone assessments in a pediatric population from the Canary Islands. Osteology, 5(1), MDPI, 6. https://doi.org/10.3390/osteology5010006
Ontell, F. K., Ivanovic, M., Ablin, D. S., & Barlow, T. W. (1996). Bone age in children of diverse ethnicity. AJR American Journal of Roentgenology, 167(6), 1395–1398. https://doi.org/10.2214/ajr.167.6.8956565
Pew Research Center. (2015, September 28). Modern immigration wave brings 59 million to U.S., driving population growth and change through 2065. Pew Research Center. https://www.pewresearch.org/race-and-ethnicity/2015/09/28/modern-immigr…
Prokop-Piotrkowska, M., Marszalek-Dziuba, K., Moszczynska, E., Szalecki, M., & Jurkiewicz, E. (2021, August 22). Traditional and new methods of bone age assessment—An overview. Journal of Clinical Research in Pediatric Endocrinology, 13(3), 251–262. https://doi.org/10.4274/jcrpe.galenos.2020.2020.0091
Schmeling, A., Garamendi, P. M., Prieto, J. L., & Landa, M. I. (2016, April). Forensic age estimation methods, certainty, and the law. Deutsches Ärzteblatt International, 113(4), 44–50. https://doi.org/10.3238/arztebl.2016.0044
Shin, N.-Y., Lee, B.-D., Kang, J.-H., Kim, H.-R., Oh, D. H., Lee, B. I., Kim, S. H., Lee, M. S., & Heo, M.-S. (2020, September 16). Evaluation of the clinical efficacy of a TW3-based fully automated bone age assessment system using deep neural networks. Imaging Science in Dentistry, 50(3), 237–243. https://doi.org/10.5624/isd.2020.50.3.237
Tanner, J. M., Healy, M. J. R., Goldstein, H., & Cameron, N. (2001). Assessment of skeletal maturity and prediction of adult height (TW3 method). The Bone & Joint Journal, 3, W. B. Saunders, 110. https://boneandjoint.org.uk/Article/10.1302/0301-620X.84B2.0840310c
Jenson, E., Jones, N., Rabe, M., Pratt, B., Medina, L., Orozco, K., Spell, L. (2021, August 12). 2020 U.S. population more racially and ethnically diverse than in 2010. America Counts, United States Census Bureau. https://www.census.gov/library/stories/2021/08/2020-united-states-popul…
United States Census Bureau. (2022, April 1). *Special edition* 1950 census records release. https://www.census.gov/newsroom/facts-for-features/2022/1950-census-rec…
Menchaca, A., Pratt, B., Jensen, E., Jones, N. (2023, May 22). Examining the racial and ethnic diversity of adults and children. United States Census Bureau. https://www.census.gov/newsroom/blogs/random-samplings/2023/05/racial-e…
UNHCR. (n.d.). Born into refugee life. https://www.unhcr.org/refugee-statistics/insights/explainers/children-b…
United Nations Committee on the Rights of the Child. (2020, November 2). Views adopted by the Committee under the Optional Protocol to the Convention on the Rights of the Child on a communications procedure, concerning communication No. 40/2018. Convention on the Rights of the Child, United Nations. https://www.icj.org/wp-content/uploads/2023/03/4.-G2027647.pdf
Visiana. (2019, October). BoneXpert clinical manual versions 3.0 & 3.1. https://bonexpert.com/manuals/BoneXpert_Manual.pdf
Yuh, Y.-S., Chou, T. Y., & Tung, T.-H. (2023, February). Bone age assessment: Large-scale comparison of Greulich-Pyle method and Tanner-Whitehouse 3 method for Taiwanese children. Journal of the Chinese Medical Association, 86(2), 246–253. https://doi.org/10.1097/JCMA.0000000000000854